Research digest // KISS1R / GPR54 agonist
Kisspeptin is the KISS1 neuropeptide that switches on the reproductive axis, one rung upstream of GnRH.
A study-attributed digest of the mechanism, the human trials, and the open questions — every quantitative claim read straight from the published literature and cited.
The short version
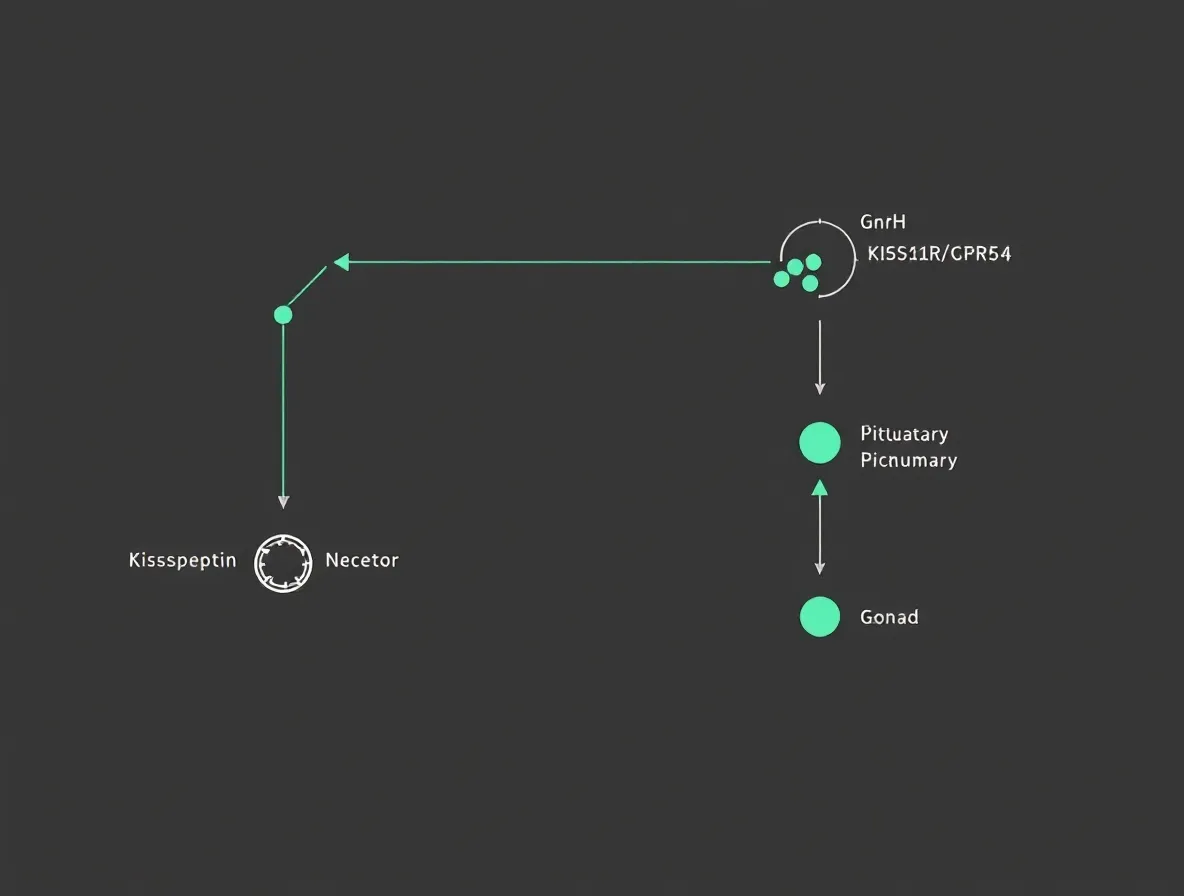
Kisspeptin is a small signaling molecule made by nerve cells in the brain. It is the "on switch" for the body's reproductive system. When kisspeptin lands on its docking site (a receptor called KISS1R, older name GPR54), it tells a second set of nerve cells to release GnRH (gonadotropin-releasing hormone) in short bursts. GnRH then tells the pituitary gland — a pea-sized gland under the brain — to send out two hormones, LH and FSH, which act on the ovaries and testes to drive ovulation, sperm production, and the sex hormones. So kisspeptin sits at the very top of that chain. It is not a sex hormone itself, and it is not a supplement. Researchers have given it to people in carefully run studies to trigger egg release in IVF, restart missing periods, and study sexual-desire brain circuits. It has no approval from any regulator for any use. What people report — including the downsides — is on the effects page.
What the Kisspeptin literature has demonstrated
Kisspeptin is the protein product of the KISS1 gene and the principal upstream activator of GnRH neurons [1]. In healthy men, an intravenous kisspeptin-10 bolus of 1 ug/kg drove luteinizing hormone (LH) from 4.1 to 12.4 IU/L within 30 minutes, and a continuous infusion raised LH pulse frequency and lifted serum testosterone from 16.6 to 24.0 nmol/L [3]. In women with hypothalamic amenorrhea — absent periods from a quietened reproductive axis — continuous kisspeptin-54 restored LH pulses roughly threefold and increased pulse secretory mass about sixfold versus vehicle [4]. As an IVF oocyte-maturation trigger, a single subcutaneous kisspeptin-54 dose matured eggs in 95% of high-risk women with no case of moderate, severe, or critical ovarian hyperstimulation syndrome (OHSS) [5]. Each of these is a controlled human finding, attributed to a stated dose, route, and population.
The through-line is mechanism. Kisspeptin acts on the body's own GnRH neurons rather than supplying any hormone directly. That single fact organizes everything else: read the kisspeptin mechanism of action first, because the upstream position explains both the breadth of the effects and the central limitation.
One rung above GnRH — and why that distinction matters
Kisspeptin is the ligand: the KISS1 gene product that engages KISS1R and relays a signal downstream. It is not GnRH, not a GnRH agonist, and not a sex steroid — it acts one step above all of them, on the neurons that make GnRH [13]. It is also not a dietary supplement, despite the search phrase "kisspeptin supplement," because every documented human dose is an investigational research protocol given under medical supervision, not a consumer product on a shelf.
The research family has two main isoforms. Kisspeptin-54 (KP-54, originally named metastin) is the 54-amino-acid form; kisspeptin-10 (KP-10) is a shorter C-terminal fragment. Both share the same Arg-Phe-amide tail needed to bind the receptor, but they differ sharply in how long they last — a point the Kisspeptin research page covers in full.
Investigational, with one defining limitation
No kisspeptin product has FDA, EMA, or other regulatory approval for any indication as of 2025 [7]. The published human work is Phase 1 and Phase 2 research, much of it from Imperial College London and collaborators, across healthy volunteers, hypothalamic amenorrhea, IVF populations, and sexual-desire studies [7].
The defining limitation is tachyphylaxis. Continuous or high-dose kisspeptin desensitizes KISS1R within days, so the LH and testosterone response fades [4]. Twice-daily subcutaneous kisspeptin-54 saw the acute LH increment fall sharply over two weeks [14]. This is why pulse timing — bolus versus continuous — matters more than dose size, and why the studies that worked best mimicked the body's own rhythm rather than flooding the receptor. The honest summary: large, reproducible effects on the hormone readouts, a clear ceiling set by receptor biology, and no Phase 3 trials or approvals yet.